Common Questions Parents Ask











About Our Clinic
The easiest way of requesting an appointment is by emailing [email protected] with a subject line “Appointment request”. You can also fill out the patient inquiry form on our website. We will get back to you within 24 hrs upon receiving your request.
We offer an annual package fee structure that covers all necessary office visits related to your child’s myopia management. The specific cost of the annual package depends on the type of the treatment, the frequency of the follow up visit, and the complexity of your child’s case. The cost of the lenses is not included in the annual fee.
Currently we only take VSP however all of the services and materials are FSA eligible.
In order to determine the most viable option for the long-term management of your child’s myopia, we perform thorough testing using special equipment to establish a comprehensive baseline for the treatment. An overview of the current available options, their safety and efficacy profiles, their applicability to your child’s scenario, as well as the time and financial investment required is provided to help you make an well informed decision.
The long-term efficacy and safety of Orthok treatment are highly dependent on the proper fitting of the lenses, which requires careful patient selection, in-depth knowledge of the lens design, as well as ample experience in troubleshooting. Consequently, Orthok treatment is usually provided by practitioners with advanced training in specialty contact lenses and often takes much longer chair time and more frequent visits. Additionally, clinics focused on managing myopic children often need to be equipped with advanced instruments such as corneal topographer, specular microscope, and optical biometer to allow accurate evaluation of the long-term myopia controlling efficacy and the safety of the treatments, all of which increase the cost of the service.
Our doctors are highly experienced in fitting and troubleshooting many different designs of Orthok lenses. The decision on the design of the lenses depends on your child’s level of myopia and astigmatism, the dynamic pupil response as well as other important factors such as the shape of the cornea of your child’s eyes.
We offer most of MFSCL brands that have demonstrated efficient myopia controlling efficacy. The considerations for the MFSCL design selection for your child are similar to those for Orthok treatment, which are the baseline myopia and astigmatism, corneal shape, pupil characteristics, as well as frequency of lens replacement.
Overall Myopia Control Strategies
There are multiple evidence-based methods for slowing down the progression of myopia. Evidence-based means that these methods have been tested in well-designed clinical trials sponsored by different institutions and conducted in various populations, and their effectiveness has been replicated consistently. Based on this, the three well-known methods for slowing down myopia progression are orthokeratology (OK) lenses, multifocal contact lenses worn during the day, and low-concentration atropine eye drops. There are also other methods, such as specially designed eyeglass frames, that have shown some effectiveness in myopia control, but they are not yet available in the North American market. It is important to note that currently there is no method that can guarantee the complete cessation of myopia progression. The available interventions can only slow down the progression compared to no intervention.
Another way of understanding this question is at what age myopia tends to stop progressing. The age when myopia is likely to stabilize depends on many factors such as the age of myopia onset, intensity of near work, and parental history of myopia etc. Note that the “projected age of stabilization” from any ocular growth chart assumes a relatively stable visual and lifestyle. In the cases of a dramatic change in visual demand (eg. studying for MCAT or LSAT), it is not uncommon to have a second phase of myopia progression after years of stable presentation.
To address the question of whether myopia can be cured, we need to consider it from two perspectives. If we define “cure” as achieving permanent clear distance vision through treatment, then it is possible to achieve a cure through laser surgery. However, myopia also has important pathological manifestations. As myopia develops, the axial length of the eye continues to increase, and this process is irreversible. The longer the eye’s axial length, the greater the tension on the retina, which becomes thinner and more prone to myopic maculopathy or retinal detachment. These risks cannot be reduced through laser surgery. Therefore, to truly control the complications associated with myopia and reduce the risk of these problems, early intervention to prevent excessive axial elongation is necessary.
No, it is not true. Myopia is the result of a combination of genetic and environmental factors. Some cases of early-onset or congenital myopia, especially those associated with other systemic issues, have a stronger genetic predisposition. However, for the more common adolescent myopia, there is ample evidence to show that its development is primarily driven by environmental factors (prolonged unhealthy visual experiences), with genetic factors playing a secondary role. Generally, the earlier myopia occurs, the more significant the influence of genetic factors, the faster its progression, and the weaker the response to various interventions in later stages. The later myopia stabilizes and develops into high myopia, the greater the risk of developing complications in the retina.
Currently, there is no direct clinical trial evidence to confirm the impact of sleep habits on vision. However, there are some suggestive findings from animal models that indicate disrupting the overall circadian rhythm may have some effect on refractive development. As the eye functions as an integrated organ, including the thickness of the cornea, choroid, intraocular pressure, and lens, all of which have their own biological rhythms, it is not surprising that disrupting these rhythms can influence the rate of eye growth. Indirect evidence from animal models suggests that staying up late and waking up late may increase the risk of myopia. However, there is no direct clinical evidence to confirm this.
If the myopia control effectiveness of OK lenses is not satisfactory, there may be several reasons for it. The most common reason is inappropriate patient selection (such as starting with a high baseline degree), improper design, or poor patient compliance, resulting in poor daytime uncorrected visual acuity. Poor daytime visual acuity can greatly affect the effectiveness of OK lenses. If this factor is excluded, a combination of low-concentration atropine or daily wear of multifocal soft contact lenses can be considered as alternatives. However, in general, the younger the age of myopia onset, the poorer the control effectiveness, regardless of the method used.
If we define myopia occurrence based on refractive status, the eye has already shown accelerated axial growth one or two years before the myopia occurs. With continuous axial elongation, the compensatory mechanisms of the eye’s refractive components (such as flattening of the anterior surface of the lens to counteract the myopic refractive state caused by axial elongation) are exhausted, resulting in the myopic refractive status. Therefore, once myopia occurs, it represents an early-to-mid stage irreversible pathological change. Additionally, whether the degree of myopia will continue to increase depends on the age of myopia onset. The earlier myopia occurs and the faster it progresses, the less likely it is to be influenced by improved visual habits. Furthermore, it is not possible to completely eliminate the causative visual habits that lead to myopia.
Myopia correction generally refers to achieving clear distance vision through the use of eyeglasses or contact lenses. This is the goal of myopia correction. The concept of myopia treatment is somewhat ambiguous in English. It can be used to refer to the methods used to control myopia because they can reduce the risk of future complications in the eye, so they can be considered a form of treatment. Therefore, the terms “myopia treatment” and “myopia control” are often used interchangeably. However, in Chinese context, “myopia treatment” is more commonly used to refer to corneal refractive surgery, which permanently eliminates myopia. Thus, the understanding of myopia treatment may vary depending on the context. Myopia control refers to a series of methods aimed at slowing down the progression of myopia and reducing the rate of axial elongation in children. The efficacy of myopia control can be evaluated through two methods: changes in refractive power (diopters) and relative axial growth rate. Physiological axial growth refers to the normal growth of the eye after birth. As a child’s height changes, the eye undergoes natural development, becoming larger and the axial length increases. Physiological axial growth does not increase the risk of complications in the eye.
Detection, Diagnosis, And Treatment
Myopia, also known as nearsightedness, occurs when the physical length of the eyeball (axial length) is relatively longer than the focal length of its refractive components (cornea and lens), causing the image of distant objects to be focused in front of the retina. Myopic individuals have better near vision than distance vision. Common early symptoms of myopia include squinting, tilting the head, frequent blinking, getting closer to objects being viewed, and experiencing blurred vision when looking at distant objects.
In most cases, myopia in children is caused by excessive axial growth of the eyeball. As the eyeball elongates, the posterior structures of the eye, such as the retina, choroid, and sclera, become thinner and more fragile, and blood supply decreases significantly. If left uncontrolled, it can lead to serious complications such as retinal detachment, retinal tears or holes, macular degeneration, and potentially irreversible vision loss. Early intervention to slow down the progression of myopia and axial elongation is crucial for preventing future complications.
Myopia cannot always be completely prevented, but early changes in visual habits may delay its onset. The younger the age of myopia onset, the lower the risk of developing high myopia. We recommend regular vision check-ups at appropriate ages, engaging in outdoor activities as much as possible, especially for children and adolescents without myopia. It is also important to avoid prolonged and close-range use of electronic devices.
- Visual acuity, including uncorrected visual acuity and visual acuity with glasses.
- Visual functions, including the ability of the eyes to adjust when focusing at different distances and the coordination of binocular vision.
- Pupillary light reflex.
- Range and accuracy of eye movements, extraocular muscle strength, control, and coordination.
- Refraction for eyeglass prescription, including subjective and objective refraction. The prescription is personalized based on the patient’s visual needs, occupation, lifestyle, etc.
- Contact lens services, assessment of visual acuity with contact lenses, prescription issuance, and updates.
- Evaluation of eye health, including intraocular pressure, visual fields, anterior segment, and fundus examination
The overall examination items are similar, but the procedures and emphasis may differ. For example, when examining children and adolescents, more attention is given to myopia progression, binocular vision function, and their impact on learning efficiency and quality of life. In contrast, adults may focus more on occupation-related vision correction and screening for age-related eye diseases.
If you notice your child squinting or consistently getting close to the TV, these may be signs of myopia. You can cover one eye at a time and observe if there is a difference or blurriness in distance vision. Sometimes children may not be aware that their vision is problematic and may not complain about unclear vision, but they may prefer to get close to the blackboard, TV, etc., to see clearly. The best way to detect myopia early in children is to have their eyes examined at the appropriate age. Additionally, there are various software applications available for children to check their vision at home, but not all of them have been validated for accuracy. Therefore, these apps can be useful for detecting changes in vision, especially when the testing distance and lighting conditions are appropriate, but they should only be used as a preliminary screening and not as a substitute for a comprehensive diagnosis.
It is important to note that refraction is only a part of the routine annual eye check-up, although many Chinese parents consider it as the sole purpose of an eye examination. However, apart from refraction, eye health and binocular vision function should also be assessed during regular check-ups. Specifically for refraction, if it is the first examination, it should include assessments of uncorrected visual acuity, objective refraction, and subjective refraction. For children, cycloplegic refraction should also be performed.
The decision to perform cycloplegic refraction is not solely based on refractive assessment but also on the detection of peripheral retinal issues that may be difficult to identify without cycloplegia. Many common retinal conditions (such as glaucoma, diabetic retinopathy, hypertensive retinopathy, etc.) are asymptomatic in their early stages and can be detected through regular examinations. For patients under 40 years of age without significant myopia and after establishing a comprehensive baseline record of retinal health, it is generally recommended to undergo cycloplegic retinal examinations every 2-3 years. For patients aged 60 and above or those with moderate to high myopia, as well as those who previously had abnormal retinal findings, it is advisable to undergo cycloplegic examinations annually. Cycloplegia performed for the purpose of paralyzing the ciliary muscle is not necessary for myopic patients with normal best-corrected visual acuity. However, for patients with other visual functional problems, the initial examination with cycloplegic results is sufficient, and there is no need for cycloplegia during every eyeglass prescription.
Generally, for the initial refractive examination of children and adolescents, cycloplegic results should be obtained for comparison. If there is no poor visual acuity or abnormal visual function, cycloplegia is not necessary to update the glass prescription each time.
In the early stages of myopia or refractive errors, there is a certain linear relationship between the degree of myopia and visual acuity without correction. Generally, within -1D (100 degrees) of myopia, every 0.25D of myopia affects visual acuity by one line. For example, if a child has normal vision, the uncorrected visual acuity would typically be 20/20. With -0.25D of myopia, the visual acuity would be around 20/25. For -0.50D of myopia, it would be around 20/30. For -0.75D to -1D of myopia, the uncorrected visual acuity ranges from 20/40 to 20/70. At this stage, there is a certain linear relationship between uncorrected visual acuity and the degree of refractive error. However, beyond -1D, there is no linear relationship between uncorrected visual acuity and the degree of myopia. For example, both a -3D and a -5D myopic patient may have a visual acuity of 20/200 without correction. Therefore, the visual acuity alone cannot be used to estimate the degree of myopia accurately.
Outdoor Activities
The exact mechanism behind the myopia-preventive effects of outdoor activities has not been definitively determined. However, numerous studies have found that adequate illumination is a crucial factor in the myopia prevention achieved through outdoor activities. One hypothesis argues for the elevated dopamine release under bright lighting. When the eyes are exposed to sunlight, a substance called dopamine is released, which can inhibit myopia development. Other studies suggest that the protective effect of outdoor activities on myopia is related to the spectral composition of the light source rather than the intensity of light. Some researchers propose that the distant focus associated with outdoor environments helps the visual system relax more fully, which is beneficial for myopia prevention. In conclusion, apart from illumination (including intensity and spectral composition), the broader field of view in outdoor environments can reduce myopia-inducing stimuli and minimize close-range eye usage, thereby delaying myopia progression. As long as it is not direct exposure to intense sunlight, reading and writing outdoors are permissible, while considering the discomfort caused by reflections from the reading material or screen.
If your child does not have myopia yet, the best way to prevent it is to increase their outdoor time. Currently, there is still insufficient research evidence regarding the optimal duration of outdoor activities during a day. However, engaging in outdoor activities immediately after near-work activities is the best way to mitigate the impact of near-work on vision. It is recommended to have at least two hours of outdoor activities per day to prevent myopia, and it should be done in small increments of no shorter than 5min and right after near-work activities.
Regardless of whether you are an adult or a child, it is recommended to wear sunglasses in environments with strong outdoor sunlight to prevent excessive ultraviolet rays from entering the eyes and to prevent early onset cataracts.
The effect of outdoor activities on myopia and the quantitative relationship between it and the intensity of light have not been established yet. Although the light intensity outdoors on cloudy days is lower than on sunny days, it is still much higher than indoor lighting.
There are no studies specifically addressing this question.
Long-distance viewing provides better visual relaxation than closing the eyes for rest. To eliminate factors that induce myopia, visual relaxation should occur in the entire visual field, not just the central area, and for a sufficient duration (at least 5-10 minutes or more). This means that even if you have a very large living room at home, the visual relaxation effect of a child in the living room cannot be compared to outdoor relaxation because even though their central gaze distance is far enough, the peripheral projection of the ceiling, floor, and furniture on the retina still creates a crowded effect, which does not provide the optimal visual relaxation. During eye closure, the retina cannot effectively experience the inhibitory light signals for myopia, so it is not an effective method for visual relaxation.
OrthoK Treatment
The safety of OK lenses is not an absolute concept but depends on various factors. Wearing any type of contact lens increases the risk of eye infections, inflammation, and injury, without exception. Ensuring the long-term safety of OK lenses mainly depends on three factors:
- Proper lens fitting (such as centering the lens, ensuring the cornea evenly bears the weight of the lens, and allowing sufficient tear exchange);
- Strict adherence to wearing and care routines;
- Regular follow-up visits to detect and address any minor issues promptly, avoiding the development of more serious complications.
If these three aspects are ensured, the long-term safety of wearing OK lenses is very high.
The risk of serious complications associated with long-term wear of OK lenses depends on several factors:
- Lens material: Comparatively, hard lens materials are safer than soft lenses. Hard lenses do not contain water, which almost eliminates the risk of pathogens breeding on the lens surface. Additionally, the fitting of hard lenses typically involves greater movement on the corneal surface, reducing the risk of pathogen adherence and subsequent infection.
- Wearing schedule:The risk of complications is lower with daytime wear compared to overnight wear. Daytime lens wear involves blinking and increased tear exchange, which improves safety. In contrast, overnight wear significantly reduces tear exchange and decreases lens movement, increasing the risk of pathogen infection.
- Fitting condition: Good lens fitting is essential, particularly for orthokeratology (OK) lens treatment. Proper patient selection, the optometrist’s expertise in lens design, and ample clinical experience are crucial factors for achieving a good fit. Patient compliance with wearing and care: Contact lenses are medical devices placed directly on the ocular surface. Rough handling, careless care routines, and forcing lens wear despite warning signs from the eyes are the main causes of complications.
If the care routine for OK lenses is mastered, it should not take more than 5 minutes per day, with 2-3 minutes in the morning and evening, but consistency is crucial. Ensuring the long-term safety of wearing OK lenses requires three elements: appropriate lens handling, meticulous care, and regular follow-up visits. Specifically, lens handling should be done with care, and care routines should be thorough. Additionally, regular follow-up visits are essential. Poor lens fitting or improper use and care can lead to serious consequences. For example, inadequate lens cleaning with deposits or biofilm formation can cause chronic inflammation, especially allergic inflammation. Severe improper care, such as failing to detect surface cracks or small defects during lens handling, can result in corneal damage when the lens is worn. Although hard lens materials are less prone to pathogen growth, if there is a thick biofilm on the lens surface due to poor cleanliness, the biofilm itself can act as a breeding ground for bacteria. Therefore, if the lens is not clean and there are micro traumas on the cornea, combined with viscous tears during overnight wear and reduced lens movement, the risk of corneal inflammation and infection increases significantly.
After wearing OK lenses, the cornea is reshaped into a unique multifocal lens. This lens ensures clear imaging in the central area of the retina, providing good daytime unaided distance vision. At the same time, the multifocal lens effect on the cornea may generate a strong “myopia control signal” in the retina, slowing down the elongation rate of the eyeball and reducing myopia progression.
The effectiveness of myopia control with OK lenses varies among individuals but, on average, it can achieve approximately 50% control. This means that in a group of children wearing OK lenses, the average axial growth rate is about half that of the same-age control group wearing regular eyeglasses.
When a child’s unaided visual acuity reaches 20/40, wearing OK lenses can provide a significant improvement in daytime unaided vision, motivating the child to comply with the treatment. The degree of myopia corresponding to a visual acuity of 20/40 can vary significantly among individuals, generally ranging from -0.50D to -1.0D. If the myopia degree is too low and the unaided visual acuity is better than 20/40, the child’s desire to wear glasses is usually not strong, and treatment compliance may be poor.
It depends on the severity of eye-related allergy symptoms. If the allergy is severe, causing significant eye redness, roughness of the conjunctiva (inner surface of the eyelids), and severe itching with constant eye rubbing, it may not be suitable to wear OK lenses, and treatment for allergies should be addressed first. For mild cases, continued lens wear may be considered, but lens care, especially the rubbing step, should be performed diligently, as individuals with allergic conjunctivitis tend to have higher protein secretion in their tears, which can form a biofilm on the lens surface. Apart from absolute contraindications for treatment (such as irregular corneas or active inflammation), OK lenses may not be suitable for patients with high degrees of myopia, small and tight eyelid fissures that make lens insertion difficult, extreme anxiety during lens handling, or poor compliance with lens use and care
The baseline age for starting OK lens treatment is generally 7-12 years old. However, being younger than this age range is not an absolute contraindication for OK lens treatment. Whether younger patients are suitable for OK lens treatment depends on various subjective and objective factors. The subjective factors mainly consider the following points:
- the child’s psychological maturity, which refers to whether they can understand the purpose of OK lenses and are willing to overcome the initial discomfort of wearing them;
- whether the child has a strong desire to wear glasses (usually a desire to be free from wearing regular glasses during the day);
- the ability to effectively communicate any problems to their parents. If a young child meets all three conditions, experienced doctors generally do not consider the child’s physiological age as an absolute indicator of whether OK lenses can be prescribed.
It is worth noting that there is no upper age limit for OK lens treatment. However, since adults have higher visual quality requirements, are more sensitive to glare, ghosting, and other visual disturbances, and have higher visual demands for nighttime driving, OK lenses are more suitable for adults with lower degrees of myopia. This is because the degree of glare and myopia reduction are positively correlated.
Regardless of the brand or design of OK lenses, the success rate of fully correcting myopia and the baseline degree of myopia are generally inversely proportional. In other words, the lower the degree of myopia, the less corneal reshaping is required, making the fitting process easier. For children with myopia below -4D, the probability of achieving a daytime uncorrected visual acuity of 20/25or higher exceeds 80%. However, for children with -6D of myopia, the probability of achieving complete correction with OK lenses is less than 50%, and there is a significantly increased risk of corneal surface micro-damage. There is no specific range of astigmatism for OK lens use. It depends on the nature of astigmatism (whether it is corneal or lenticular in origin), the influence of corneal shape on lens fitting, the impact of residual astigmatism on uncorrected visual acuity, the patient’s expectations, lens design choices, and the doctor’s experience, among other factors.
OK lens treatment is a long-term and continuous method of myopia management. The complexity of fitting, the special nature of corneal reshaping and overnight lens wear, and the long-term nature of treatment make the careful selection of an OK lens doctor and clinic particularly important. Additionally, OK lens treatment can be costly, so it is important for parents to have comprehensive communication with the doctor regarding treatment expectations, costs, and other important factors to ensure mutual agreement. When signing the fitting agreement, it is crucial to read it carefully, clarify any doubts, and then sign it. Specifically, the selection of an OK lens doctor should primarily consider the following factors:
- Relevant experience and knowledge of the fitting doctor
- Ability to communicate effectively with children
- Difficulty in scheduling appointments on weekends
- Clinical equipments necessary to monitor for the efficacy and safety of the treatment
- Transparency of fees
The annual cost of OK lenses can vary significantly among different clinics. Generally, the initial fitting cost for OK lenses in the first year ranges from $2000 to $2500, and the cost of lens materials itself is between $500 and $800 per pair. It is important to emphasize that the fee structure for OK lenses differs between the United States and other countries. In most U.S. clinics, the service fee for OK lens treatment (including the doctor’s time and expertise) and the cost of lenses are separate. Additionally, there may be costs associated with related care products.
Regular follow-up visits for OK lenses are crucial. The first follow-up visit after overnight lens wear is generally scheduled as early in the morning as possible, and it requires the child to wear the lenses for examination to detect any fitting issues or subtle corneal damage that may have occurred during overnight lens wear. If the first follow-up visit goes well, wearing the lenses during the weekly follow-up may not be necessary. However, if any issues are identified during the first follow-up, lens adjustments may be needed, and the child may be asked to wear the lenses during the weekly visit for observation before removing them at the clinic.
There can be several reasons for temporarily suspending OK lens wear, with the most common one being poor lens fitting. If the lenses become increasingly misaligned over time, it may be necessary to have the child stop wearing them for a few nights to allow the cornea’s eccentric shape to return to a state that won’t affect the fitting of the next lens. This is the most common reason for temporary suspension. Additionally, if there is any damage to the corneal epithelium, it may be necessary to stop wearing the lenses to allow the cornea to fully repair before resuming lens wear. Long-term suspension, which is the most severe and least desirable situation, can occur due to the occurrence of corneal infections. Even if a corneal ulcer fully heals and there is no scarring on the corneal surface, most doctors do not recommend resuming lens wear. In addition, if OK lenses are not effectively controlling myopia or if there are other reasons leading to poor daytime visual correction, the doctor may recommend alternative options.
There is currently no definitive answer regarding whether there is a rebound effect on myopia control after temporarily stopping OK lens wear. One reason is that after stopping OK lens wear, myopia may increase due to the corneal curvature rebounding (gradually becoming steeper from a flattened state caused by reshaping). This process can last for several months or even over a year. During this lengthy period, it is challenging to accurately quantify whether myopia worsens due to corneal shape restoration or if it is due to the combination of corneal shape restoration and accelerated axial elongation. Additionally, if OK lenses are stopped prematurely (i.e., before myopia has completely stabilized), axial elongation may continue, but this represents ongoing myopia progression rather than rebound after stopping lens wear. In summary, there is currently no reliable evidence to support the notion that stopping OK lens wear leads to rebound myopia development.
Clinical trials are currently underway to study the synergistic effects of combining orthokeratology or spectacle lenses with atropine eye drops for myopia control. This approach may be suitable for children with rapidly progressing myopia, high degrees of myopia, or children with both parents being myopic. Currently, optical and pharmacological interventions used in animal models have shown some additive effects, but the exact mechanisms underlying the synergistic effects are not yet fully understood.
There is a possibility, but it is extremely rare. OK lens materials themselves are quite resilient, so lens fragmentation usually occurs when external forces act on lenses that already have noticeable defects (such as deeper or longer scratches on the surface). In such cases, the most fragile part of the lens may shatter under significant pressure and end up inside the eye. However, at the same time, the cornea has strong resilience, and in the case of fractures in gas-permeable lens materials, severe irreparable cuts to the cornea are generally unlikely to occur.
Contact lens care systems for OK lenses can be broadly divided into multipurpose solutions and hydrogen peroxide systems. Multipurpose solutions usually contain surfactants (for rubbing the lens, removing deposits), disinfectants (to eliminate microbial pathogens on the lens surface), conditioning agents (to enhance lens surface wetting), and other additional components such as buffering salts. Multipurpose solutions are very convenient to use, as they combine lens rubbing, rinsing, and soaking functions in one solution, usually without the need for additional products. Hydrogen peroxide solutions are care systems that use 3% hydrogen peroxide as the active ingredient. These solutions require special lens cases or enzymatic additives to neutralize hydrogen peroxide in a timed and measured manner. Hydrogen peroxide solutions have excellent antimicrobial properties, particularly against fungi and Acanthamoeba. Additionally, when completely neutralized, the solution does not cause eye irritation due to preservatives when it comes into contact with the ocular surface. The main limitation of hydrogen peroxide solutions is the need for neutralization, and once (soft) contact lenses are placed in the solution, they cannot be immediately removed and worn, as it can cause intense irritation. Thus, hydrogen peroxide solutions are not suitable for situations such as removing lenses for daytime napping. It is important to note that when using hydrogen peroxide solutions, the step of rubbing and rinsing the lenses with the solution should not be omitted. While hydrogen peroxide solutions effectively kill microbial pathogens, they cannot ensure thorough removal of lens surface deposits through soaking alone.
Currently, there is no randomized controlled clinical trial providing evidence of different designs of OK lenses having differential effects on myopia control. Most clinical studies reporting better myopia control effects for a particular brand are retrospective in design, which means they selectively analyze a subset of cases from a larger sample. Retrospective studies have a high risk of sampling bias, so the results obtained can only provide reference for future prospective studies with larger sample sizes and cannot establish a causal relationship. It is important to note that the selection of a suitable brand or design should not be the decision of the parents but rather the prescribing doctor, based on the patient’s specific condition, the doctor’s experience with different designs, and their understanding of various options. The doctor’s choice of brand depends on several factors: their familiarity with a particular brand/design, knowing its potential and how to adjust parameters in case of any issues; the warranty period provided by the manufacturer, as some brands offer more flexibility in parameter adjustments within a certain period; and the cost of the lenses. These factors are considered by the doctor, and it is not the role of parents to select the brand.
There could be two reasons for this. First, when replicating an exact copy of a lens, there are around twenty parameters, but the prescription record provided to parents or documented in the case may only include seven or eight of them. Therefore, having the same values for these parameters does not guarantee that the new lenses will have the exact same shape as the previous ones. The second reason is related to the individual patient’s lenses. After wearing lenses for a long time, the lenses and the cornea have undergone a certain degree of adaptation. When new lenses with the same parameters are fitted, the lens shape is actually slightly different from the lenses worn for two years. These subtle changes in lens shape can lead to a decrease in visual acuity (similar to the difference in sensation between well-worn shoes and a new pair of the same model).
The visual acuity with lenses and without lenses during an OK lens examination reflects different aspects of OK lens wear. The lenses themselves have power, so visual acuity with lenses is influenced by the fit of the lenses and the shape of the cornea. On the other hand, post-treatment unaided visual acuity (without lenses) is only affected by the cornea’s shape after OrthoK treatment. There is no direct relationship between the two. Good visual acuity with lenses does not necessarily mean good unaided visual acuity, and poor visual acuity with lenses does not necessarily mean that the desired unaided visual acuity cannot be achieved. The evaluation should be made in consultation with the prescribing doctor.
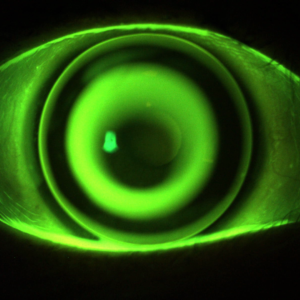
An ideal OK lens fitting should meet three main principles:
- an appropriate lens diameter,
- good centration on the cornea, and
- adequate movement, especially after the overnight wear, as lens binding to the corneal surface significantly increases the risk of microbial keratitis.
- Parents can try wearing contact lenses themselves to have a firsthand experience, which can help them assist their children better.
- Explain to the child the pros and cons of wearing OK lenses and establish realistic expectations.
- Communicate with other children who are already wearing OK lenses and encourage them to share their experiences.
The use of topical anesthesia can make the initial wearing experience more comfortable for both the child and the parent. However, topical anesthesia only numbs the surface of the cornea. The feeling of foreign body sensation when wearing OK lenses primarily arises from the friction between the lens and the upper eyelid, rather than the cornea’s sensation. This foreign body sensation cannot be completely eliminated by topical anesthesia. Therefore, many children still experience some degree of foreign body sensation even with topical anesthesia. The main benefit of topical anesthesia is its psychological comforting effect to alleviate anxiety. Importantly, after the use of topical anesthesia, the child’s perception of the normal baseline sensation during initial lens wear is affected. When they encounter foreign body sensations at home, they may struggle to differentiate between normal sensations during initial wear and discomfort caused by inadequate lens cleaning or improper insertion technique, which can hinder problem-solving abilities. Although the use of topical anesthesia is ultimately the doctor’s decision, it does not significantly increase the success rate of initial lens wear.
The assessment of OK lens positioning cannot be accurately evaluated without a professional slit lamp biomicroscope. Most parents’ notion of the “correct position” may refer to whether the lens is placed on the cornea or if the lens and the iris (cornea) form a perfect concentric relationship. There is a significant difference between the curvature of the cornea and the conjunctiva, a translucent layer overlying the sclera (white portion of the eye). If the OK lens is completely misaligned and ends up on the sclera instead of the cornea, which is much flatter, the lens is likely to be stuck onto the sclera. In such cases, the lens cannot be repositioned on the cornea by blinking or pushing it with a finger. Therefore, if the entire lens is stuck on the sclera, it needs to be removed, cleaned, and rechecked. Once it is confirmed that there are no issues with the lens, it can be reinserted. However, if a part of the lens is placed on the cornea during insertion, even if it is slightly off-center, as long as the parameters are appropriate, the lens will eventually find its correct position on the cornea (and automatically reset). Closing the eyes or performing gentle maneuvers does not significantly aid in the lens resetting process. Once a portion of the lens is on the cornea, it will reset whether you blink or close your eyes.
If we compare contact lens rewetting drops from over 10 years ago to artificial tears, they had clear differences in their formulations, so they couldn’t be used interchangeably. Nowadays, the formulations of contact lens rewetting drops and artificial tears have become increasingly similar, but for safety reasons, it is still better to use artificial tears in conjunction with OK lens wear. As a filling solution for OK lenses before insertion, it is advisable to avoid using high-viscosity products (such as gels) or lipid-based artificial tears (such as Optive Mega-3) as they can interfere with lens fitting or lead to more deposits on the lens surface.
In principle, during the acute phase of eyelid meibomian gland inflammation (hordeolum), OK lens wear should be discontinued. However, after the acute phase, if the lump is very small, without redness, pain, tenderness, obvious secretions, and there is no discomfort while wearing the OK lens, and normal vision is restored after removing the lens, it is permissible to continue wearing the lens with the doctor’s approval.
Hydrogen peroxide has a significant toxic reaction to the corneal epithelial cells, so when it comes into contact with the eyes, it feels like getting pepper spray into the eyes, causing an significant stinging sensation. Fortunately, the toxic reaction caused by hydrogen peroxide on the corneal epithelium generally recovers completely within 24 to 48 hours, and it does not cause any permanent damage to the eyes. Apart from the initial discomfort, there should not be any other major issues.
If the lenses are thoroughly rubbed every day, using Progent (AB solution) once every quarter is sufficient to effectively remove deposits from the lens surface.
The effect of OK lenses on myopia control varies greatly among individuals. Most children using OK lenses still experience some degree of axial elongation. Whether it is due to suboptimal lens design can only be determined after specific examinations. The exact degree of myopia correction with OK lenses cannot be accurately measured, so the claim of an annual increase of -0.25 diopters may not be reliable. The control effect needs to be evaluated comprehensively by a combined review of the changes in axial length, refraction over the lenses, and the patient’s age.
Firstly, it’s important to clarify the concept of myopia control effectiveness. It is not a binary measure (yes or no), but rather a spectrum that quantifies the degree of effectiveness. Based on several clinical trials, orthokeratology (OK) lenses have been shown to reduce axial elongation by approximately 50%. But what does 50% mean? For example, if children wearing single-vision eyeglasses experience an average annual increase in axial length of 0.3mm, and those wearing OK lenses show a 0.15mm increase, this represents a 50% control effect.
However, two key points must be considered. First, there is significant individual variation in the effectiveness of OK lenses for myopia control. While the average reduction is 50%, the standard deviation is quite large. Some children may wear OK lenses for many years with minimal changes in prescription or axial length, while others may not achieve the average control effect observed in clinical trials. This does not necessarily indicate a lack of effect, as it is impossible to determine the extent of myopia progression without any myopia control intervention in that same patient.
The fitting of OK lenses is a critical factor influencing the control effect. Simply wearing OK lenses does not guarantee the same outcome for everyone. If the lens parameters are not properly chosen or if corneal reshaping is insufficient, the child may experience poor uncorrected visual acuity during the day. Prolonged periods of poor vision can significantly stimulate axial elongation, thereby reducing the control effect of OK lenses.
In addition to proper OK lens fitting, the proportion of genetic factors involved in a child’s myopia progression is a significant determinant of effectiveness. Generally, the earlier the onset of myopia in a child, the higher the contribution from genetic factors, the faster the progression, and the poorer the response to interventions. This conclusion holds true for all myopia control methods, including OK lenses, multifocal soft lenses, and atropine eye drops.
It’s important to note that using OK lenses doesn’t eliminate the influence of a child’s visual habits on myopia progression. Good eye hygiene, sufficient visual relaxation, and outdoor activities are still essential for myopia control.
If a child only has myopia without other issues such as strabismus or large difference between two eyes’ prescriptions, the likelihood of developing amblyopia is very low. If a child is diagnosed with amblyopia along with -3.00 diopters of myopia, it is advisable to seek a second medical opinion to exclude other factors that may cause poor visual acuity.
No, OK lenses only inhibit non-physiological axial elongation caused by poor visual environments. Eye development and axial elongation accompanying bodily growth (especially height) do not increase the risk of retinal diseases. Whether the axial length continues to increase after discontinuing OK lens wear primarily depends on the intensity of eye usage. Although the plasticity of eye shape decreases with age, and the rate of axial elongation slows down, the protective effect of age is not absolute. There are cases in adult myopic individuals where, due to a period of high-intensity eye usage, worsening of myopia resumes after many years of stability.
Dry spots are not a specific description, so the diagnostic significance is limited. If there is a feeling of dryness after wearing OK lenses, it is important to first exclude micro-injuries to the corneal epithelium caused by fitting issues or lens defects. The use of artificial tears can help alleviate dryness, but it is crucial to address corneal epithelial damage caused by fitting or lens issues fundamentally, rather than relying solely on artificial tears to relieve symptoms.
The clarity of vision can be assessed objectively and subjectively. Objectively, if a patient wearing OK lenses can achieve 20/30 or better in one eye by the afternoon or before going to bed, it is generally considered clinically acceptable. This level of clarity does not significantly affect the effectiveness of myopia control treatment. Subjectively, the perception of clear vision depends on the child’s individual visual needs and age. For children around seven to eight years old, their overall visual demands may not be very high, so even if the objective visual acuity is the same, they may not perceive it as blurry. However, for a teenager who has just started driving, the same level of visual acuity may cause noticeable glare at night and affect driving confidence. Therefore, subjective visual clarity depends on the age and specific visual demands of the wearer.
The ideal time for follow-up appointments depends on the main purpose. In the initial phase of OK lens fitting (within the first 1-2 weeks of wearing), follow-up appointments primarily focus on:
- evaluating the lens fit;
- checking for any adverse reactions of the cornea and conjunctiva;
- assessing the daytime unaided visual acuity; and
- ensuring proper lens care.
Considering these factors, it is easier to observe lens fit issues and minor corneal injuries in the morning. Minor corneal injuries repair rapidly, and if they have already healed by the afternoon examination, the doctor may not be able to detect these subtle conditions. Therefore, in general, we recommend morning follow-up appointments on the first day and first week of lens fitting.
After entering the stable phase of fitting, follow-up appointments focus on:
- checking for any regression in daytime visual acuity;
- monitoring myopia/axial progression; and
- evaluating any changes in fitting.
During this phase, afternoon appointments are more effective in detecting visual regression and other issues. As axial length exhibits biological rhythmicity, regular check-ups every quarter should be scheduled at similar times to ensure the comparability of biometric data.
Overall, in the initial phase, morning appointments are recommended, while subsequent check-ups offer more flexibility. However, if parents or children subjectively feel that their vision is better in the morning compared to the afternoon, it is advisable to have the appointment in the afternoon to assess the adequacy of vision during those times.
The sensation of the lenses and their movement reported by parents or experienced by children themselves after lens wear is not a highly accurate indicator of ideal lens fitting. The most important indicators are the dynamic evaluation during lens wear with fluorescein staining in the clinic and the corneal topography and eye health assessment after lens removal, which are the most accurate and objective indicators. It is normal for lenses to exhibit different levels of movement or sensations between the left and right eyes even in cases where both eyes are well-adapted. However, if the lenses are poorly fitted, resulting in one lens blinking off the eye with every blink or one lens frequently moving while the other remains stable, these situations do indicate fitting issues. In general, subjective sensations such as lens movement or foreign body sensations are not reliable indicators of the quality of lens fitting.
Not necessarily. Different lens designs can result in different sensations when removing the lenses. Typically, if the baseline myopia is higher and requires more significant corneal reshaping, the lens design tend to have a higher level of vaulting around the cornea, meaning the lens fits tightly against the cornea. In such cases, lenses can be more challenging to remove, especially in the morning. The difficulty of lens removal depends on various factors, including specific techniques, the presence of corneal injuries after lens removal, and the overall effectiveness of the reshaping. However, in general, it is common for lenses to fit tightly in cases of astigmatism or relatively high degrees of myopia.
The parameters for OK lens fitting depend on the shape of the child’s cornea and the baseline level of myopia and astigmatism. To achieve the desired fitting effect, it is important for the lens to have excellent centration and good mobility. These factors are mainly related to the corneal curvature, and sufficient flattening of the central cornea is also necessary. The degree of flattening depends on the level of baseline myopia. In other words, the higher the myopia before starting lens wear, the greater the force required for corneal shaping in the central cornea. Other considerations include the child’s sleep duration, whether they experience significant visual regression from morning to evening, and whether they need clear vision between 8 PM and 10 PM but experience visual regression. In some cases, it may be necessary to wear the OK lenses a few hours before bedtime to compensate for insufficient overnight sleep. In such cases, in addition to the degree of corneal shaping on the posterior surface of the lens, it is important to have clear and comfortable vision when wearing the lenses. If the lens power is not designed properly, it is possible to achieve sufficient corneal shaping, but the visual comfort may be compromised. Therefore, OK lenses themselves have a prescription. However, the correlation between the lens power and corneal shaping is not necessarily direct. Two lenses can have identical corneal shaping effects on the posterior surface, but the anterior surface curvature may be different, resulting in the same corneal shaping effect but different visual outcomes for the wearer. To sum up, OK lenses do have a prescription, which is also related to the shape of the child’s cornea. The need for replacement depends on the stability of the prescription and the condition of lens care.
If the uncorrected visual acuity of the myopic eye is worse than 20/40, wearing OK lenses can significantly improve vision and increase the child’s willingness to wear them. However, if the uncorrected visual acuity of the myopic eye is still relatively good, (e.g. 20/30 in each eye), and the child does not perceive a significant improvement in vision with OK lenses, their willingness to wear the lenses may be limited. Additionally, consideration should be given to the prescription of the other eye. Generally, fitting OK lenses for one eye only requires the child to understand that OK lenses not only correct vision but also have a role in controlling myopia progression. If the child does not grasp this concept and relies mainly on the other eye for distance vision, they may not see a significant benefit from wearing OK lenses, leading to poor compliance.
- Regular visual acuity checks: Assess the visual acuity of both eyes while wearing the OK lenses.
- Corneal topography: Monitor corneal shape and changes to ensure the lenses fit properly and are not causing any adverse effects on the cornea.
- Slit-lamp examination: Check the health of the cornea, conjunctiva, and other anterior eye structures.
- Intraocular pressure measurement: Monitor intraocular pressure to ensure it remains within a normal range.
- Refraction: Regularly evaluate the refractive status of the eyes to determine any changes in prescription.
- Follow-up consultations: Schedule regular follow-up appointments with the eye care professional who prescribed the OK lenses. These appointments allow for discussions about treatment progress, adjustments to the lens fitting if needed, and addressing any concerns or questions related to the treatment or eye health.
Increased redness of the eyes can occur after wearing OK lenses, especially during the initial adaptation period. This is mainly due to corneal molding and tear film changes caused by the lens. To prevent or minimize this discomfort, it is important to follow proper lens care and hygiene practices, such as:
- Ensuring the lenses are properly cleaned and disinfected before insertion.
- Using lubricating eye drops as recommended by your eye care professional to maintain a healthy tear film.
- Avoiding wearing lenses for extended periods without breaks.
- Keeping the lenses and lens case clean to prevent contamination.
Significant redness associated with OK treatment warrants prompt consulting with the eye doctor.
Punctate epithelial staining is a common occurrence in OK lens wearers. Mild, superficial punctate staining usually does not require discontinuation of lens wear or specific treatment. However, if the staining becomes more significant or is associated with discomfort, it is important to consult with an eye care professional for appropriate management and guidance. Note that the severity of epithelial defect may not be correlated with that of the symptoms. Whenever in doubt, consult with your eye doctor.
Multifocal Contact Lens
Continuous overnight wearing of soft contact lenses (wearing them during the day and night) is the primary risk factor for corneal infections and inflammation. If you forget to remove your lenses before sleeping, it is recommended to remove them immediately upon waking up and allow your eyes sufficient rest time. It is advisable not to wear contact lenses the following morning or for the entire day. If you experience symptoms such as redness, eye pain, sensitivity to light, tearing, or any other discomfort after removing the lenses, it is important to contact your optometrist or ophthalmologist promptly. It’s worth noting that overnight wearing (e.g., in the case of orthokeratology lenses) and continuous overnight wearing of soft lenses are two completely different wearing patterns. Orthokeratology lenses are usually removed in the morning to ensure the cornea has sufficient time without the lens during the day, whereas continuous overnight wearing of soft lenses means the cornea remains covered by the lens during both daytime and overnight sleep, resulting in different risks of inflammation and infection.
The care solution for soft lenses can be used for rinsing hard lenses, but it cannot effectively maintain the surface wetting properties of rigid lenses as dedicated care solutions for hard lenses do. Most of the rigid lens care solutions are too viscous and are not suitable for cleaning and soaking soft lenses.
Multifocal soft contact lenses, such as Misight 1d, not only correct vision and provide clear distance vision but also effectively slow down the progression of myopia (nearsightedness). Regular single-vision contact lenses do not have the ability to control myopia progression.
Currently, there is no direct comparison between multifocal soft contact lenses and orthokeratology lenses in the same study population regarding their effectiveness in myopia control. Based on the average myopia control effects in the experimental groups, these two methods show similar effectiveness. However, there is a greater individual variability in myopia control with orthokeratology treatment.
Both methods are suitable for many myopic children and teenagers. The choice between the two methods depends on various factors such as the patient’s age, degree of myopia, corneal shape, lifestyle, and environment. A thorough examination (including refraction, corneal topography, biometry, assessment of ocular health, etc.) should be conducted, followed by a systematic analysis with your doctor to determine the best option.
Contact Lens Cleaning
Regardless of the type of contact lens material or wearing mode, the basic care steps usually
include the following:
- Rubbing: Rubbing is a crucial step in contact lens care, as it is the simplest, most
convenient, and effective way to remove deposits from the lens surface. The formation
of a biofilm on the lens surface significantly increases the risk of allergies during long-
term wear, leading to reduced comfort. Moreover, the biofilm provides an ideal growth
base for pathogens, and failure to remove it increases the risk of eye infections during
lens wear. - Rinsing: Thoroughly rinsing the lens ensures the complete removal of deposits dislodged
during the rubbing step, so it should be done after the rubbing process. - Soaking: Soaking the lenses with specialized care products effectively disinfects them
and restores the surface wetting properties of the lens.
The above three steps have different purposes and cannot replace each other.
Contact lens care system can be generally classified as multi-purpose system and hydrogen
peroxide system.
In general, multipurpose solution formulations contain surfactants (to facilitate rubbing and
removal of deposits from the lens surface), preservatives (to eliminate pathogenic
microorganisms from the lens surface), conditioning agents (to increase lens surface wetting),
and other additional ingredients such as buffering salts. Multipurpose solutions are very easy to
use and combine the functions of rubbing, rinsing, and soaking the lenses, usually without the
need for additional products.
Hydrogen peroxide solution is a care system with 3% H202 as the active ingredient. It generally
requires a special lens case or enzyme solution to be added to the care solution to achieve
timed and quantified neutralization of the hydrogen peroxide. Hydrogen peroxide solution has
excellent antimicrobial properties, particularly effective against fungi and acanthamoeba,
surpassing the disinfection capabilities of multipurpose solutions. Additionally, after thorough
neutralization, the care solution does not cause eye irritation due to preservatives when it
comes into contact with the eye surface.
Soft contact lenses have a certain water content, typically ranging from 30% to 70%, which sets
them apart from hard lens materials. Additionally, the porous network structure of soft lens
materials allows care products’ components to be absorbed into the lens material.
On the other hand, hard contact lens materials do not contain water, and the material matrix has
very small pores. Care solution components remain only on the lens surface and do not
penetrate into the depths of the lens.
Due to the differences in materials, soft and hard contact lenses also have different
requirements for care products. Soft contact lens care solutions need to use very gentle
preservatives so that the care solution that penetrates into the lens structure does not cause
strong irritation when released onto the eye surface. At the same time, hydrogen peroxide must
be completely neutralized before the lens can be used.
In comparison, hard contact lens care solutions require better conditioning properties to ensure
long-term surface wetting of the lens. Therefore, the formulation of hard lens care solutions is
often more viscous than that of soft lens care solutions. When using hydrogen peroxide for hard
lenses, there is no need to wait for complete neutralization. Simply rinse off the remaining
hydrogen peroxide on the lens surface before wearing.
OK lenses use materials similar to daily wear rigid gas permeable lenses, but there are some
differences in the care due to the distinct wearing pattern and the fitting status with the cornea.
- Due to the overnight wearing mode, Orthok are more prone to developing biofilm on the
lens surface compared to daily wear rigid lenses. This is because during nighttime sleep,
the lipid and protein secretion in tears is higher than during daytime. - As the eyes are closed during sleep, tear exchange is reduced, making it more likely to
have biofilm formation on the lens surface.
Therefore, the rubbing step is especially important for thoroughly removing the deposits on the
lens surface. For wearers who is prone to develop biofilm relatively quickly, considering the use
of a strong cleaning agent for rubbing the lenses and regularly employing enzymatic cleaning
agents to remove protein deposits from the lens surface is advisable.
Plasma treatment is a purification process applied to the surface of hard contact lens materials with the aim of enhancing surface wetability and wearing comfort. New lenses that have undergone plasma treatment are not suitable for use with abrasive cleaning agents containing micro-particles, as such formulations may accelerate the dissipation of the plasma treatment effect.
Progent (AB solution) utilizes a strong oxidative reaction generated by the combination of two formulations to break down protein and lipid deposits, such as biofilm, on the surface of contact lenses. This process facilitates the complete removal of deposits from the lens surface. For wearers who have poor compliance with the daily lens rubbing step or are prone to developing biofilm for various reasons, Progent treatment can be considered every 2-3 months. However, once the AB solution is mixed, it produces a strong bleaching effect, so prolonged soaking of the lenses in the solution can cause discoloration. Therefore, each soaking session should not exceed 30 minutes.
Using artificial tears in conjunction with OK lenses serves two main purposes:
- Before applying the lenses, instilling a drop of AT on the lens can prevent excessive air
bubbles from accumulating between the lens and the cornea, which may otherwise
affect the lens molding effect and visual acuity after lens removal.
Prior to removing the lenses in the morning, using AT can help increase the lens movement and
reduce the risk of damage to the cornea caused by lens adhesion.
Artificial tear products come in various formulas, often leading parents to feel overwhelmed and
faced with decision-making difficulties. Here, we provide a few basic factors as the main criteria
for making a choice:
Common types of AT formulations include solutions, gels, emulsions, or ointments, which are
selected based on their intended use. For OK lens wear, solution is preferred to avoid deposit
formation on the lens, which could affect comfort, visual acuity, or corneal molding. Additionally,
some AT products are specifically designed for patients with poor Meibomian gland function,
characterized by reduced lipid secretion in their tears. For children wearing OK lenses, it is
advisable to avoid using lipid-based formulations to prevent lipid film formation on the lens.
Solution Viscosity: AT products often contain viscosity agents to prolong their retention on the
ocular surface. When using AT in conjunction with OK lenses, it is not advisable to use
formulations that are excessively viscous.
Preservatives: Since Orthok treatment is a long-term process, the safety of using AT on the
ocular surface is crucial. Some newer smart preservatives (which are effective in the packaging
but break down upon contact with the eye are safer for the ocular surface compared to
traditional preservatives like BAK. If financially feasible, preservative-free artificial tear
formulations are considered more ideal.
Low Dose Atropine
Common side effects of long-term use of low-concentration (0.01% to 0.05%) atropine include light sensitivity, blurred near vision, and transient redness of the eyes after instilling. Most side effects are mild and do not significantly affect treatment compliance, but the higher the concentration, the more pronounced the side effects may be. The specific duration of use varies from person to person, but low-concentration atropine is intended for long-term use in myopia control, and there are no reports in the literature suggesting any irreversible adverse reactions resulting from long-term use.
There is a clear dose-response relationship between atropine concentration and myopia control. The higher the concentration used, the better the myopia control during treatment. However, higher concentrations also present two issues. First, higher concentrations result in more pronounced side effects during treatment, with the most common being light sensitivity and blurred near vision. Second, higher concentrations, especially with longer treatment duration, may lead to a noticeable rebound effect during the 3 to 6 months after discontinuation. Rebound refers to a period when myopia and axial elongation progress faster than before using atropine. Therefore, when using higher concentrations for a longer duration, it is important to gradually reduce the dosage and frequency before discontinuation, allowing the body enough time to adjust. Currently, the commonly used starting concentrations are 0.025% and 0.05%. If after observing for 6 months to a year the control effect is not satisfactory, it may be necessary to increase the concentration. In North America, the highest concentration commonly used is 0.05%, while in Asia, especially in Taiwan and Singapore, concentrations of up to 0.1% or even 0.25% are used.
“Rebound” refers to a period after discontinuing atropine where the degree of myopia and the rate of eye axis elongation exceed the rate before treatment. The two main factors influencing rebound are the concentration used and the duration of treatment. The most effective way to reduce rebound is to gradually reduce the dosage. The higher the concentration used and the longer the treatment duration, the more gradual the tapering process should be. Generally, there are two approaches to gradual reduction. One approach is to maintain a single concentration but decrease the frequency of instillation, such as changing from nightly to every other night, then to three times a week, and further to twice a week. This method reduces the concentration in the eye by reducing the frequency of instillation. The other approach is to decrease both the frequency and concentration simultaneously. For example, if currently using 0.05% concentration, it can be reduced to 0.02%, and then to 0.01%. Both of these tapering methods are commonly used.
It is not uncommon to experience some level of light sensitivity with LDA treatment. The higher the concentration and the more frequently the dosing regimen, the higher the chance and severity of the symptom. Whether it should be discontinued is a balanced decision between the severity of the light sensitivity and the potential benefit in myopia control and whether there is a viable alternative option to consider. Wearing photochromic glasses or applying the eye drop in early evening (rather than right before bedtime) may help alleviating the symptoms.
Currently, the exact mechanism of how low-concentration atropine precisely controls myopia is not fully understood. However, several points are known. Firstly, the control of myopia with atropine is not directly related to its effect on pupil dilation and accommodation. Secondly, the primary targets of atropine may be more concentrated in the posterior part of the eye, but whether it acts on the retina, choroid, or sclera is still unclear. It is worth noting that eye drops are not the most targeted administration route, and the effective dose that reaches the posterior part of the eye is very low, with significant individual differences. The suitability and tolerance of atropine concentration vary among individuals.
If the stinging sensation occurs only in one eye after using the eye drops, it is highly unlikely to be caused by the medication itself. In most cases, the irritation due to the formulation of the eye drops tend to affect both eyes similarly. Therefore, if one eye experiences more discomfort, it is possible that there are other underlying issues in that eye, such as conjunctivitis or corneal epithelial damage. These conditions can increase sensitivity to stimuli, resulting in a stinging sensation after instillation. If such symptoms occur frequently, it is advisable to promptly consult your doctor for an examination.
The safety of long-term use of low-concentration atropine is well-documented. Large-scale clinical trials in Singapore have conducted long-term follow-up studies and statistics for over ten years, and no serious adverse reactions have been reported following prolonged use. Currently, there are at least three different concentrations and formulations of atropine undergoing pre-market clinical trials in the United States, and we look forward to more accurate information related to their approval in the near future.
The shelf life of compounded low-dose atropine (LDA) eye drops is relatively short, typically around 30 days. Few studies have explored the stability or batch-to-batch consistency of these compounded preparations. To maximize their efficacy, it is recommended to store the eye drops in the refrigerator, consistent with storage practices used in clinical trials.
Clinical trials on atropine for myopia prevention are still ongoing, and the final results are not yet conclusive. However, if both parents are myopic, especially if they have high myopia, and if the child shows signs of age-appropriate insufficient farsightedness reserve or if monitoring reveals a rapid increase in eye axis length, such as an increase of 0.2mm in half a year, even if myopia has not yet developed, these indications strongly suggest a high probability of myopia occurrence in the near future. In such cases, it is advisable to proactively start using low-concentration atropine for preventive purposes.
If the goal is to delay the onset of myopia, atropine is more practical because orthokeratology lenses are only suitable for children who already have myopia. If a child has already developed myopia, optical methods should be the first choice, with atropine used as a secondary treatment. Optical treatments include wearing orthokeratology lenses overnight, using multifocal soft contact lenses during the day, or using newly designed optical frame lenses (currently limited to certain countries and regions).
It is possible that low-concentration atropine can affect intraocular pressure. Before starting low-concentration atropine treatment, the patient’s baseline intraocular pressure and angle of the anterior chamber, which is the angle between the cornea and the iris, should be checked. In cases where the angle is very narrow, instillation of atropine may cause an increase in intraocular pressure. Therefore, the use of atropine, regardless of the concentration, should be guided and monitored by a doctor after a comprehensive evaluation and regular follow-up examinations.
Slit lamp examination is a common method for assessing the width of the anterior chamber. If necessary, anterior segment optical coherence tomography (OCT) can provide a quantitative evaluation of the chamber’s morphology. Since most children have a normal anterior chamber, doctors usually do not specifically emphasize this finding during routine examinations, which may cause unnecessary concerns among parents.
Wearing sunglasses does not affect the effectiveness of outdoor activities in myopia prevention and control. There is currently no evidence suggesting that sunglass wear reduces the efficacy of LDA in myopia control.
Different doctors may have different opinions on similar cases. In this situation, the author would choose to treat the myopic eye with atropine first. This is because if atropine is used in the non-myopic eye on the opposite side, it would increase the near-work load, which could further burden the already myopic eye and increase the stimulus for myopia development. A comprehensive evaluation of the child’s refractive status, differences in eye axis, and visual function is necessary to provide a safe and effective atropine treatment plan.
Other Approaches for Myopia Management
Currently, several newly designed spectacle lenses have shown promising results in myopia control in manufacturer-sponsored clinical trials. However, the reproducibility of these results must be validated through independent studies before the treatment can be widely recommended for real-world patient populations. While these glasses are not yet approved in the U.S., if your child has been prescribed them elsewhere, we are fully equipped to provide ongoing management to monitor both the safety and effectiveness of the treatment.
When myopia reaches a level that significantly affects uncorrected visual acuity, wearing glasses should be initiated. It is recommended to wear glasses full time (both for distance and near) once the level of myopia is greater than -2.0D. Prolonged blurry vision can accelerate the progression of myopia.
There is currently no definitive evidence to support the effectiveness of image defocus in preventing and controlling myopia. Although there are some studies and theories regarding these methods, their efficacy and practical feasibility are still controversial.
Visual Hygiene
Currently, there is no specific scientific research directly addressing this aspect. However, some related studies have found that the viewing distance from the screen is more important than the type of screen. When the screen is closer, the eyes need to exert more effort to focus, which can cause visual fatigue. When the viewing distance is closer, there is greater harm to vision during the same duration of visual activities. Therefore, when comparing electronic products, such as tablets, iPads, iPhones, and other smartphones, they are more harmful than television when used for the same amount of time. It is beneficial for children’s vision to avoid prolonged close-distance work as much as possible.
In terms of inducing and developing myopia, there is no absolute safe distance for using electronic devices. In general, the closer the working distance, the greater the intensity of eye focusing within the same duration, and more likely it is to cause visual fatigue. Therefore, the further the eyes are from the screen, the lighter the visual system’s load during the same duration of close-distance work. It is recommended to place the computer or iPad on a table to avoid working at a close distance.
For watching TV, a distance of at least 3 meters is recommended. It is advised to take a 5-10 minute break every 30-45 minutes of viewing, and it is preferable to spend the break time outdoors rather than engaging in other close-range visual activities.
For children, it is recommended to take a 5-10 minute break every 30-40 minutes, as this provides a good opportunity to reduce the continuous effects of stimuli that contribute to myopia development. During breaks, it is preferable to be outdoors rather than engaging in other close-range work. Researchers found that children who spent recess time outdoors had a lower prevalence of myopia compared to those who stayed indoors.
It has been reported that under similar reading difficulty conditions, the average reading distance on an iPad or Kindle is closer to the reading distance of printed books, and the reading efficiency is lower compared to printed books. Therefore, in terms of the same reading time, printed books have a slightly lower risk of visual fatigue and myopia compared to electronic devices. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8557948/
Currently, there is no consistent evidence showing that blue light has a protective or worsening effect on myopia. Blue light can affect the color and perceived comfort of screens. You can also adjust the screen display through software and apps such as f.lux, which can change the screen’s color according to the time of day, reducing blue light in the evening as it can affect sleep and circadian rhythms. There is no strong evidence showing that blue light-blocking lenses help slow down axial elongation of the eyes.
The earlier children are exposed to electronic devices, the greater the risk of myopia. Younger age groups are more susceptible to myopia-inducing factors affecting the retina and rapid eye axial growth. While electronic devices may have constructive effects on brain development, in terms of myopia risk, it is advisable to minimize children’s exposure to electronic devices during early stages.
There is limited research on the impact of motion-sensing games on vision, particularly regarding the harm related to myopia development. However, it has been found that playing such games requires prolonged and intense focusing, which has been identified as a risk factor for myopia. It is recommended to limit the duration of playtime to no more than 30 minutes per session, followed by a 20-30 minute break.
If the fundamental cause of dry eyes is poor meibomian gland function, which leads to an imbalance in tear components, then warm compresses or steam eye masks can help alleviate dry eyes. Visual fatigue is related not only to prolonged close-distance work but also to poor tear film quality. If the tear film is unstable, it affects the overall image quality of the eye as an optical system. Therefore, improving tear film quality can be helpful for reducing visual fatigue.
There is no reliable evidence indicating that color inversion has a controlling effect on myopia.
Vision Health Light Sources
RLRL uses a 2mW red laser light source, which falls under the Class 3R laser devices and has similar light energy to laser pointers. Before discussing its effectiveness in myopia control, the focus should be on its safety, especially in terms of long-term and repetitive use and safety while fixating on the fovea centralis. Currently, there is limited safety assessment for the use of “Bo Guan Yi,” so it is not recommended for use in children and adolescents. Slowing down axial elongation at the risk of permanent macular damage is not worth it.
Currently, there are indeed studies suggesting that excessive use of LED lighting may affect human circadian rhythm and sleep quality, among other things. Therefore, low color temperature lighting may have certain benefits. However, there is no direct coherence between low color temperature light sources and visual health or improvement in sleep quality for patients, nor can it directly control or prevent myopia.
No, personally, I believe that comfort is the most important factor.
Visional Health Supplements
There are many over-the-counter eye drops available to relieve eye fatigue. Most of them work by improving the quality of the tear film to alleviate eye discomfort. Currently, besides low-concentration atropine eye drops prescribed for delaying myopia progression, there are no other eye drops proven to effectively prevent myopia.
There is currently no large-sample clinical trial evidence supporting the use of intraocular pressure-lowering drugs in myopia of moderate to low degrees during the early stages of myopia. However, for high myopia, especially when myopia continues to progress in adulthood, doctors may consider prescribing intraocular pressure-lowering drugs. This is because at that stage, the scleral tissues are already significantly stretched and the axial length of the eyeball is increased. In this situation, the use of intraocular pressure-lowering drugs may have dual benefits: first, reducing the development of the eye and expansion of the eyeball due to intraocular pressure itself, and second, as high myopia and high intraocular pressure have a cumulative effect on the risk of glaucoma, the use of intraocular pressure-lowering drugs may also help reduce the risk of glaucoma to some extent.
Dopamine (medication) has shown good results in myopia control in animal models through intravitreal or posterior segment injections. However, there is no data available regarding the sufficient absorption of dopamine eye drops by the posterior segment tissues of the eye to achieve effective and safe myopia control.
Omega-3 and anthocyanins are primarily considered as health supplements at present. There is currently no evidence, either from animal models or clinical trials, supporting their effectiveness in myopia control.
Literature reports a correlation between the severity of myopia in children and their dietary habits and BMI, but there is no causal relationship evidence, as both phenomena may be the common result of a lack of outdoor activities. Long-term intake of high-carbohydrate foods increases the risk of developing diabetes, which has a significant impact on vision and ocular health.
No, if a child’s diet is relatively balanced, oral fish oil does not provide any additional benefits. In the case of older individuals, especially those with a possible family history of age-related macular degeneration, they may benefit from omega-class supplements. However, there is no evidence to support their protective effect on myopia development and progression.